Supervised learning has become one of the most transformative techniques in modern healthcare, enabling early disease detection, risk stratification, and clinical decision support.
supervised learning, models are trained using labeled patient data such as diagnosis codes, lab results, symptoms, genomic markers, medical images, or EHR entries to learn meaningful patterns that correlate with specific health outcomes.
By analysing these associations, algorithms can predict the likelihood of diseases before symptoms fully appear, support physicians with objective insights, and optimize treatment pathways.
In recent years, supervised learning applications have expanded significantly due to the availability of large-scale clinical datasets, advancements in AI architectures, and an increasing push toward preventative care.
From predicting diabetes onset using lifestyle and metabolic data to identifying cancerous lesions through medical imaging, supervised models are playing a critical role in reducing diagnostic errors and improving patient survival rates.
Techniques such as logistic regression, decision trees, random forests, gradient boosting, and deep neural networks have become core analytical tools for disease prediction tasks.
However, applying supervised learning in healthcare requires strict adherence to clinical validity, fairness, interpretability, and ethical constraints.
Since incorrect predictions can directly impact patient well-being, models must undergo careful validation using clinically representative data.
Additionally, healthcare datasets often contain imbalance, noise, missing values, and bias, making preprocessing and model selection essential steps of the pipeline.
Ultimately, supervised learning allows healthcare professionals to make evidence-based decisions and deliver more personalised, timely, and accurate care.
Predictive Modeling with Supervised Learning in Healthcare
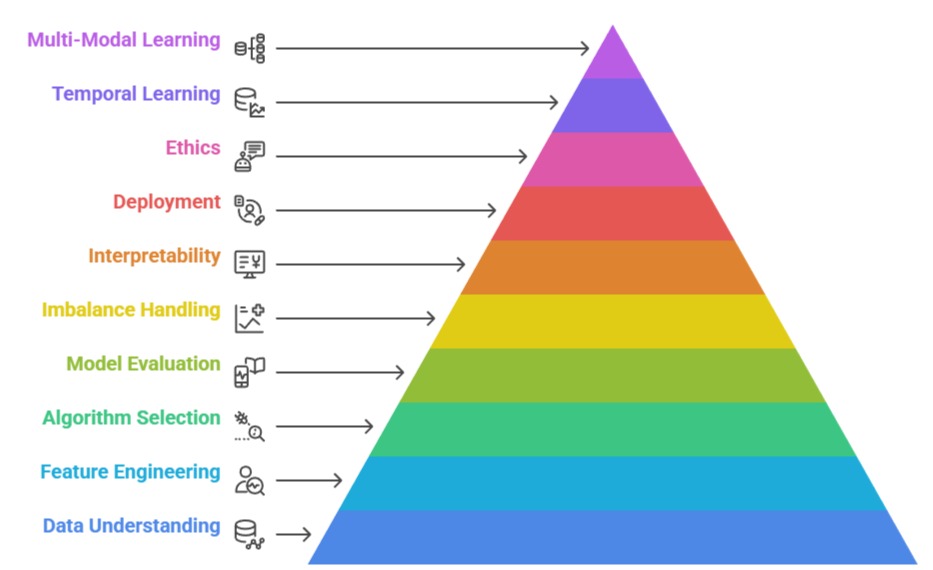
1. Understanding Labeled Healthcare Data for Prediction
Supervised learning depends on high-quality labeled data such as diagnosis codes (ICD), pathology reports, lab test values, radiology labels, and physician-verified outcomes.
In healthcare, label accuracy is crucial because mislabelled cases can mislead the model and result in clinically unsafe predictions.
Data must therefore undergo cross-checking with EHR logs, clinical notes, and validated disease registries.
Class labels often include binary outcomes like “disease / no disease,” risk category levels, or multi-class diagnoses.
Creating and curating these labels requires collaboration between clinicians and data teams.
As healthcare data is heterogeneous, models must learn from structured, semi-structured, and unstructured sources simultaneously. This makes careful labeling and feature extraction one of the most important steps in disease prediction.
2. Feature Engineering from Clinical Variables
Feature engineering is crucial for extracting meaningful patterns from patient data, especially because many risk factors like age, comorbidities, or lifestyle indicators strongly influence disease probability.
In healthcare datasets, features may come from vital signs, medication history, imaging metrics, blood test biomarkers, genomics, or patient-reported symptoms.
Transformations such as normalization, encoding categorical clinical data, and resolving temporal dependencies are essential to improve model accuracy.
Clinically inspired features such as lab score thresholds (e.g., HbA1c ranges) or interaction effects between demographic and medical variables often enhance predictive performance.
Robust feature engineering helps convert raw medical data into a form that reflects underlying biological relationships, improving both accuracy and interpretability.
3. Choosing Appropriate Supervised Algorithms
Algorithm selection depends on disease type, predictor complexity, dataset size, and interpretability needs. Logistic regression and decision trees are preferred in early prototyping and clinical settings due to their transparency and simplicity.
Random forests and gradient boosting machines provide stronger predictive performance for complex datasets while managing noise and nonlinearity.
Deep learning models such as neural networks excel in imaging-based disease prediction, especially for cancer detection, radiology segmentation, and pathology slide analysis.
Healthcare practitioners often require interpretable outputs, so explainability-oriented models or hybrid approaches are used. Choosing the right algorithm ensures both clinical reliability and practical usability in real-world hospital workflows.
4. Model Training, Validation, and Clinical Evaluation
Training supervised models in healthcare requires careful validation techniques, such as stratified cross-validation, to maintain population diversity and balanced disease representation.
Metrics like AUC-ROC, sensitivity, specificity, F1 score, and predictive value are essential because clinical decisions depend heavily on minimizing false negatives.
External validation using patient cohorts from other hospitals ensures generalizability and reduces overfitting. Models must also undergo evaluation by clinicians to verify whether predictions align with medical reasoning and real-world patterns.
Clinical trials, retrospective studies, and regulatory frameworks (FDA/EMA) play a role in validating high-risk prediction models. This multi-step evaluation process ensures that predictive models are both scientifically valid and clinically safe.
5. Handling Imbalanced Disease Classes
Most healthcare predictions involve diseases that occur far less frequently than healthy cases, such as cancer, rare disorders, or acute emergency events. Imbalanced datasets can cause supervised models to ignore minority disease classes, leading to dangerously inaccurate predictions.
Techniques such as SMOTE oversampling, class-weighted loss functions, threshold tuning, and ensemble methods help improve sensitivity for rare disease cases.
Meanwhile, careful validation ensures that artificial balancing does not distort true clinical patterns. Addressing imbalance is essential for ensuring fair diagnostic support, reducing bias, and catching early-stage disease cases that might otherwise be missed.
6. Interpretable Supervised Models for Clinical Trust
Healthcare professionals must understand how a model reaches its predictions—making interpretability a core requirement.
Techniques like feature importance scoring, SHAP values, LIME explanations, and decision path tracing help clinicians validate whether predictions make biological and medical sense.
Interpretable models reduce the “black box” effect, allowing hospitals to adopt AI systems more confidently. Transparent reasoning also helps identify biases, data errors, and clinically improbable correlations.
Clinicians and data scientists must collaborate regularly to refine explanations and ensure alignment with clinical logic. Interpretability ultimately ensures safety, regulatory approval, and physician trust.
7. Real-World Deployment and Clinical Integration
Deploying supervised models in healthcare requires robust integration into EHR systems and clinician workflows. Predictive outputs must be delivered through dashboards or alert systems that fit seamlessly into daily hospital operations.
Additional monitoring is needed to track model drift, data quality changes, and new treatment protocols that may affect accuracy.
Human-in-the-loop frameworks ensure clinicians make the final decision while using model predictions as supportive insights.
Deployment also involves cybersecurity measures, privacy compliance (HIPAA/GDPR), and continuous auditing. Real-world integration transforms theoretical models into practical tools that directly improve patient outcomes.
8. Ethical Considerations for Disease Prediction Models
Supervised learning in healthcare must prioritize fairness, patient privacy, and clinical accountability. Models trained on biased datasets may systematically disadvantage certain demographic groups, leading to inequitable care.
Safeguards such as bias detection tools, representative sampling, and fairness-aware algorithms are essential. Ethical oversight ensures models do not replace clinician judgment but rather enhance decision-making.
9. Temporal and Longitudinal Supervised Learning
Many diseases evolve over time, making temporal modeling critical for tasks like predicting hospital readmission or disease progression.
Supervised models that incorporate time-series features or sequential patterns produce more clinically realistic predictions. This allows healthcare teams to anticipate complications proactively.
10. Multi-Modal Supervised Learning in Healthcare
Modern supervised learning can combine data from multiple sources—EHRs, wearables, imaging, genomics, and clinical notes.
Multi-modal models offer richer insights and significantly higher prediction accuracy.
This approach is increasingly used in oncology, cardiology, and personalized medicine.
